Hello Dr. Winget
Thanks for taking the time to answer my questions and do this interview. So, I wanted to take this opportunity to both learn and inform my readers about cardiovascular health. Since I try to interview experts in the field that also take exercise seriously, I thought of no better person than yourself for this topic. And guys, if you have ever seen Dr. Winget in the weight room, you will know what I mean when I say that he is an animal. We’re talking full pull ups, push ups, jump squats in circuits that will make you sweat just watching him. On top of that he is a tennis player and I hear you can catch him on running on Spear Street quite often. The man lives a fitness lifestyle.
AB: Could we start with you telling us a little about yourself? What you do, your educational background and your specialties?
JW: Andrew, thanks for a much for asking me to participate in this interview. It has been a pleasure getting to know you this past 6 months or so.
I am an Associate Professor of Medicine, at the University of Vermont, College of Medicine. I attended Denison University and graduated with a bachelor of arts in computer science in 1981. I attended medical school at Tufts University, School of Medicine in Boston and graduated in 1986. I was an internal medicine resident, chief medical resident and cardiology fellow at UVM from 1986-1993. Since 1993, I have been an attending cardiologist.
My specialty is cardiovascular diseases. This includes treating patients with coronary artery disease, congestive heart failure, hypertension, valvular heart disease, congenital heart disease, and arrhythmias.
I see stable outpatients in the Cardiovascular Clinic on Tilley Drive in South Burlington. I take care of hospitalized patients primarily at Fletcher Allen Healthcare. I travel to Rutland Regional Medical Center 2 days per month. I see patients at Porter Medical Center in Middlebury, VT one day per month.
AB: What kind of patients do you see on a regular basis?
JW: I primarily see patients with cardiovascular problems.
AB: In your opinion what are the top factors that contribute to cardiovascular disease?
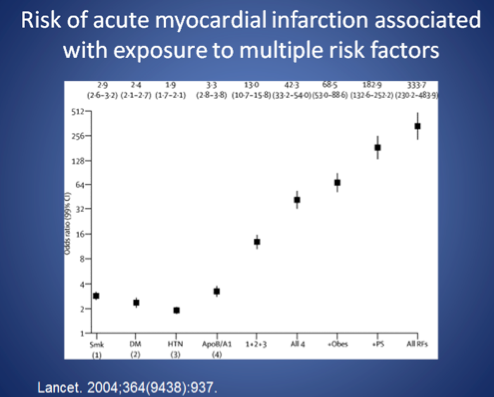
JW: The Framingham Study is an ongoing longitudinal study of 5000 inhabitants of Framingham, MA which started in the 1950s. From this study, we discovered that the major risk factors for coronary artery disease are smoking, high blood pressure, diabetes, high cholesterol and a family history of early coronary artery disease. The more risk factors you have, the higher the risk of developing cardiovascular disease.
The slide below shows the risk of having a heart attack based on the number of risk factors. This is expressed as an odds ratio. An odds ratio of 2 means that an individual has twice the risk. Notice how quickly the odds ratio increases. If an individual has 4 major risk factors then their risk is approximately 50 times higher than an individual with no risk factors.
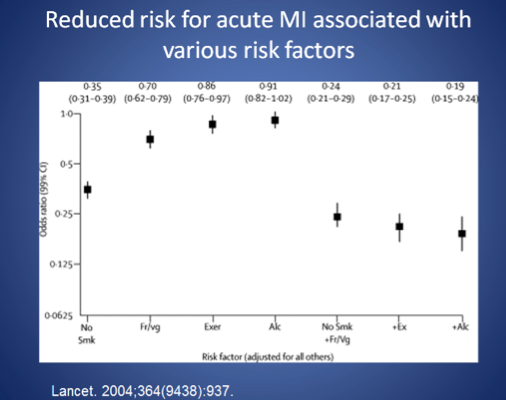
The next diagram demonstrates how the risk of heart attack is reduced by not smoking, eating fruits and veggies, regular exercise and moderate alcohol consumption.
AB: Using percentages or any way that you would like to describe it, how much would you say cardiovascular disease is related to genetics and how much would you say is related to poor lifestyle factors? Could you list the top poor lifestyle factors that you see?
JW: In my opinion, 75% of cardiovascular disease is acquired. 25% of cardiovascular disease is genetic and unavoidable.
Poor lifestyle choices which lead to cardiovascular disease include:
- Physical inactivity
- ObesitySmoking
- Poor dietary choices including,
- Low intake of fruit and vegetables
- High intake of sugar and highly processed carbohydrates
- Soda and snack foods
AB: Are there different sets of concerns towards cardiovascular and heart health when it comes to men and women? If so, could you please talk about this.
JW: The #1 killer of men and women in the United States is cardiovascular disease. The risk factors are the same for men and women. However, men and women do not necessarily have the same symptoms. Men tend to have more “classic” symptoms of chest pain. Women have less “classic” symptoms. Older individuals have less classic symptoms that younger people. I would remind people to discuss their symptoms with their physician / healthcare provider. Women do present with heart disease later in life compared to men.
AB So, in the research I have done, it seems that inflammation and not cholesterol levels is the problem when in comes to cardiovascular and heart health. From what I understand, cholesterol is essential to many body functions such as steroid hormone synthesis, bile production, brain function as well as being an integral part of all cells. So we absolutely need cholesterol in my opinion. I believe that the key inflammatory markers to be aware of are insulin (from chronic overconsumption of carbohydrates), homocysteine, and C-reactive protein levels. Am I correct in this thinking? If not, please correct me.
JW: It has been known for several decades that high cholesterol levels are associated with elevated risks of coronary artery disease (CAD). However, we now know that CAD takes years/decades to form. The most recent hypothesis suggests that arteries are injured in some manner. Inflammation plays a key role in vessel injury. Once the artery is injured an atherosclerotic plaque forms. Atherosclerotic plaques can then acutely rupture and cause a heart attack.
You are absolutely correct that cholesterol is essential to multiple bodily functions as you have noted above. Remember there are several different types of cholesterol in the body. The total cholesterol is made up of triglycerides, HDL (good cholesterol) and LDL (bad cholesterol). LDL particle size is also very important (small particles are bad). In general, for many Americans, LDL cholesterol levels are high and HDL cholesterol levels are low. Higher levels of LDL cholesterol, small LDL particle size, elevated triglycerides and low HDL levels are all lead to CAD.
Inflammation does play a key role in the development of coronary artery disease. Inflammation causes vessel injury which subsequently can lead to atherosclerosis. Markers for inflammation include C-reactive protein, insulin and homocysteine levels.
In general, markers of inflammation, high cholesterol levels and elevated insulin levels are all interrelated. They occur in the same patient quite often. This constellation of biochemical findings is referred to as the “metabolic syndrome”.
AB So, in the research I have done, it seems that inflammation and not cholesterol levels is the problem when in comes to cardiovascular and heart health. From what I understand, cholesterol is essential to many body functions such as steroid hormone synthesis, bile production, brain function as well as being an integral part of all cells. So we absolutely need cholesterol in my opinion. I believe that the key inflammatory markers to be aware of are insulin (from chronic overconsumption of carbohydrates), homocysteine, and C-reactive protein levels. Am I correct in this thinking? If not, please correct me.
JW: It has been known for several decades that high cholesterol levels are associated with elevated risks of coronary artery disease (CAD). However, we now know that CAD takes years/decades to form. The most recent hypothesis suggests that arteries are injured in some manner. Inflammation plays a key role in vessel injury. Once the artery is injured an atherosclerotic plaque forms. Atherosclerotic plaques can then acutely rupture and cause a heart attack.
You are absolutely correct that cholesterol is essential to multiple bodily functions as you have noted above. Remember there are several different types of cholesterol in the body. The total cholesterol is made up of triglycerides, HDL (good cholesterol) and LDL (bad cholesterol). LDL particle size is also very important (small particles are bad). In general, for many Americans, LDL cholesterol levels are high and HDL cholesterol levels are low. Higher levels of LDL cholesterol, small LDL particle size, elevated triglycerides and low HDL levels are all lead to CAD.
Inflammation does play a key role in the development of coronary artery disease. Inflammation causes vessel injury which subsequently can lead to atherosclerosis. Markers for inflammation include C-reactive protein, insulin and homocysteine levels.
In general, markers of inflammation, high cholesterol levels and elevated insulin levels are all interrelated. They occur in the same patient quite often. This constellation of biochemical findings is referred to as the “metabolic syndrome”.
AB: Talking about dietary advice now, I emphasize a diet that is high in animal proteins, complete with plenty of saturated fats coming from these animal sources as well as fats coming from sources such as coconut oil, whole eggs, and avocado. Along with this I emphasize the need for plenty of green leafy vegetables at almost every meal with fruits thrown in as well. I try to recommend organic and grass-fed when ever possible if the budget allows. As far as carbohydrates go, I tend to place the majority of them around exercise time when I feel the body most adequately can utilize them for energy and glycogen replenishment. What are your thoughts about this as a professional?
JW: I think there are several healthy diets. The diet you described above is certainly a healthy diet particularly for individuals involved in intense physical exercise. The emphasis on lean protein, whole eggs, avocado, leafy green vegetables and fruit sounds like an NFL/NHL/Major League Soccer training table.
I take care of patients who typically are not healthy. For them, I recommend a calorie and carbohydrate restricted diet with unlimited amounts of vegetables. I also recommend nearly unlimited fresh or frozen fruit. I recommend my patients consume nuts, avocado, and lean meats. Fish is an outstanding source of animal protein. It is rich in omega-3 oils which are cardio-protective. If your budget allows grass fed beef is preferable to grain fed beef.
I urge my patients to avoid “white” foods. This includes rice, wheat, and potatoes. I also urge my patients to cook their own meals.
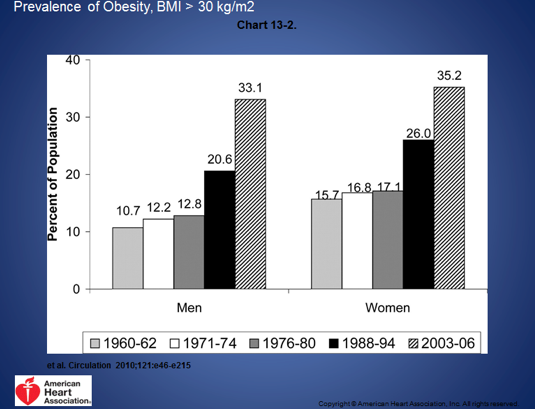
The medical community used to recommend a low-fat diet. However, over the past 40 years the prevalence of obesity has tripled. The diagrams below document this finding.
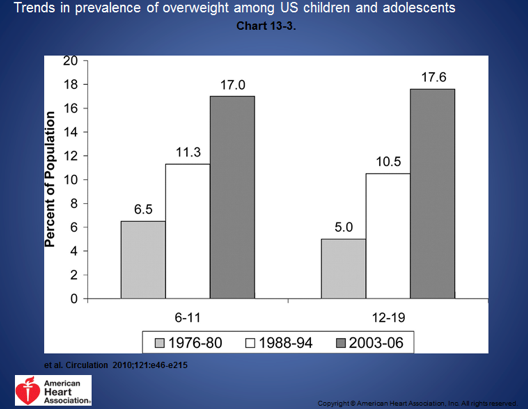
If you look at random pictures from the New York Times from 1914 compared to random pictures in the New York Times in 2014 you will be struck by the differences. People have become dramatically larger. In my opinion, this is due to diet and lifestyle.
Over the past 40 years individuals have been consuming more calories. In 1970 the average American consumed approximately 2000 calories per day. Now, the average American consumes approximately 2500 calories per day. The percentage of fat and protein in the diet has decreased while the percentage of carbohydrate has increased. These dietary changes have led to a tripling of obesity rates in this country over the past 50 years.
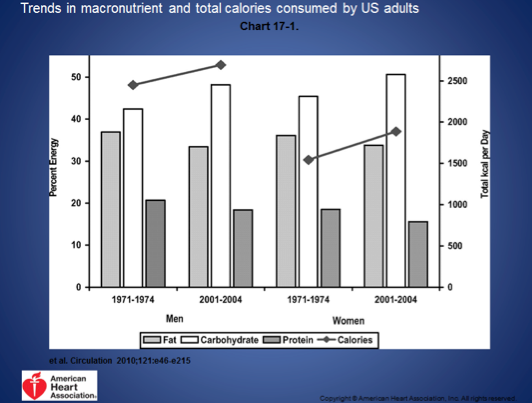
With an increase in obesity rates there has been an expected increase in diabetes, high cholesterol and hypertension. Not surprisingly, the rates of cardiovascular disease had increased also.
AB: You take exercise seriously. Can you tell about your regimen and how you got into exercise? Do you recommend any particular type of regimen to your patients?
JW: I have always enjoyed exercising. I have never been a particularly talented athlete. In fact, I have “average” athletic ability. That said, exercise has been an important part of my life which I take very seriously.
JW: Currently, I run 10-15 miles per week. 3 days a week I do a “cross fit” routine. Three mornings a week, I play singles tennis.
I do not think it matters what type of exercise you do. What matters is that you do it regularly and that you enjoy it. If you do not have fun and exercise becomes a chore then it is going to be difficult to maintain. I encouraged my patients and colleagues to vary their exercise regimen.
AB: One least question, both you and myself have both read the book Wheat Belly by fellow cardiologist Dr. William Davis, in fact you were the one that told me to read it. I found it to be an eye-opening book on the dangers of wheat consumption and I learned a great deal. Despite not really eating wheat products as a byproduct of my own dietary way of thinking, it has made me avoid wheat at all costs for myself and my clients. What, in your professional opinion, are the take home messages that you got from reading the book?
JW: Take home messages:
- There is an obesity epidemic in America
- Americans over-consume wheat based carbohydrates
- A number of diseases are linked to excessive wheat consumption such as celiac disease, migraines, acne, diabetes, cardiovascular disease, etc…
- Eliminating wheat consumption can, in some cases, reverse these diseases
- After reading Wheat Belly, I changed my dietary habits to avoid wheat.
- I also advise my cardiac patients to read the book and follow the diet.
AB: I think I took up enough of your time. Is there anything you would like to add to this interview?
JW: Thank you for allowing me to participate in your blog. Keep up your good work in nutrition counseling and athletic training
AB: Thanks for taking the time to inform both my readers and myself. I really admire a guy that can practice what he preaches, so know that the hard work you put in at the gym does not go unnoticed.